

- 12:57:00 AM
- 0 Comments


notes:
This is not my own link. I copy and paste it here from a websites called HOUSE OFFICER WORKSHOP MALAYSIA to share with you all. You can directly go to the websites and download other books here.
- 8:33:00 PM
- 0 Comments

notes:
This is not my own link. I copy and paste it here from a websites called HOUSE OFFICER WORKSHOP MALAYSIA to share with you all. You can directly go to the websites and download other books here.
- 8:30:00 PM
- 0 Comments

Hope this helps to guide you through the course somehow. I find it quite useful and helps me a lot during my posting as a medical student in the hospital.
notes:
This is not my own link. I copy and paste it here from a websites called HOUSE OFFICER WORKSHOP MALAYSIA to share with you all. You can directly go to the websites and download other books here.
- 8:28:00 PM
- 0 Comments

Orthopaedic is the branch of surgery concerned with conditions involving the musculoskeletal system. Orthopedic surgeons use both surgical and nonsurgical means to treat musculoskeletal trauma, spine diseases, sports injuries, degenerative diseases, infections, tumors, and congenital disorders.
This is a useful book for your guidance in this posting. It helps me and my friends a lot.
notes:
This is not my own link. I copy and paste it here from a websites called HOUSE OFFICER WORKSHOP MALAYSIA to share with you all. You can directly go to the websites and download other books here.
- 8:24:00 PM
- 0 Comments

POST END POSTING EXAM - LONG CASE
Fuhhh, I just told you guys that I don't want stroke patient this morning right? Turn out I went to see my patient and suddenly my patient that I got is a stroke patient. WOW. What a case... I almost broke into tears and I became very nervous. Thank God, Liyana was there helping me out to prepare for the case. She did all the research while I try to memorise and smoothing my CNS physical examination flows.
Nina was there too and helping me out with the physical examination. I'm blessed to have friends like them. My subgroup-mates also very supportive and wish me luck with the patient.
I went to Mahsuri ward at 2.00 pm and starting to clerk the patient. Then I receive a message from Dr. Ong that I need to clerk Bed 15 instead Bed 2. I asked her for confirmation, and she said Bed 15 for me. Mann..
I called my friend and I told her our case had been swapped - giving her hints that she need to read about CNS examination and ischaemic stroke 2ry to cardioembolism instead CVS case.
He came due to left upper and lower limb muscle weakness.
My case - The CVS patient
The CNS CASE
The patient was a 65 year old malay gentleman but seems old from his age. He has underlying Chronic Rheumatoid Heart Disease, Chronic Kidney Disease and Gouty Arthritis.He came due to left upper and lower limb muscle weakness.
My case - The CVS patient
My patient was well cooperate and very friendly. 1 hour was not enough for me to clerk and did my examination (suprisingly!). 1 hour given to me was always enough before this, I wonder if changing my style by first listening to all the patient had to say is better than while listening I should jotted down everything and arrange it all together. Hmm. The latter seems better for me.
My patient was a 43 year old, malay gentleman working as hawker and live in Melor, Kota Bharu. He is a smoker with history of 21 pack years for more than 30 years. He stopped smoking last month.
Patient is a known case of hypertension and also hypercholesterolnemia. He was diagnose with hypertension since 2 years ago and not compliance to medication. His hypercholesterolnemia was diagnosed last month and claimed compliance to medication.
His main complaint was chest discomfort, breathlessness and lethargy. Then nothing. Aiyoo. There was 5 days history admission to CCU recently (last month) due to almost similar presentation but worsen than the current one. He was not aware of the diagnosis. But listening to his description about the symptoms is more likely like acute myocardial infarction or acute heart failure.
Upon physical examination, Apex beat was not displace (5th intercostal space, mid-clavicular line), there was thrills present at left sternal edge. Pansystolic murmur was heard best heard by diaphragm at mitral area and radiated to axilla - bloody hell it was mitral regurgitation! And I was so pleased with myself that I can finally differentiate the type of murmur. Bibasal crepitation was heard and there was no sacral and pedal edema.
My differential diagnosis were Acute Coronory Syndrome and also Heart Failure. Dr. Ong asked me about the investigation I would done and management for Acute Coronary Syndrome Disease. She gave me good mark, Alhamdullilah !
Investigation I would carry out :
1) FBC - looking for any infections from total white count and looking for anemia from Hb level.
2) Coagulation Test
3) Renal profiles
4) Liver Function Test
5) Cardiac Biomarkers - Troponin & CKMB
6) ECG - ST elevation in Myocardial Infarction
7) Chest X-Ray - to look for any cardiomegaly or other underlying disease
8) Echocardiogram - To see the LVEF status, cardiac wall, cardiac contractility and to confirm mitral regurgitation
Management:
1) Airway
2) Breathing
3) Circulation
4) Give oxygen if patient still breathlessness
5) Primary PCI
6) Anti-fibrinolytic such as streptokinase or ateplase
7) Anti hypertensive drug - Frusemide
8) Educate patient
💕 READ HOW TO DIFFERENTIATE MURMURS 💕
HERE
- 6:55:00 PM
- 0 Comments

Long case exam is just in few hours from now and I'm so nervous about it. What if I got stroke patient? OMGG me,myself will be having stroke in front of the patient. I hope Dr. Ong will give me a straightforward case and I'm able to tackle that case too, in shaa Allah. Ease all my journey today ya Rabb.
So last night I was revising about CVS examination and got confused all over the topics. Like, WTH am I reading for the past 1 hour then got forgot again. Allahu my brain... *sigh*
Having difficulty in differentiating type of murmurs while auscultate a patient? Don't worry, you're not the only one ! Me too having the same problem since I was a 3rd year medical student. During that time, I was at Hospital Tanah Merah and I did not came across any patient with murmur. Cases were limited as it is a district hospital. All severe cases will be referred to Hospital Kota Bharu. So, I'm here now in Kota Bharu as a 4th year medical student. So many patient with interesting physical findings and most of them have murmur! YAY.
So here some tips I learnt from my prof and also from hospital specialist. One of my prof blog about it - A Simplified Approach to Cardiac Murmurs For Medical Students. And it is very helpful for me and makes my life easier. A bit confused in beginning but later you'll be okay.
From the blog:
The basic principles are:
- if the murmur coincides with the first heart sound, it is a systolic murmur.
- If it doesn't coincide with the first heart sound, it is a diastolic murmur.
Sometimes, even if you have done your best and listened while palpating the pulse, and you are still not sure whether it is a systolic or diastolic murmur, well, in the exams, you can guess and you have a fifty-fifty chance of getting it right (or wrong).
If you had to guess, then go for systolic murmurs as they tend to be:
- more common
- easier to hear compared to diastolic murmurs which tend to be low-pitched
Of course when guessing, there is a chance one might be wrong. Rather have no answer, sometimes it is better to guess.
For the sake of simplification, I memorised, as a medical student, four of the more common murmurs:
- Mitral regurgitation
- Aortic stenosis
- Mitral stenosis
- Aortic regurgitation
Here the best part about my prof. She summarised it all like this:
Mitral regurgitation is a pansystolic murmur that is heard loudest at the apex, heard through out the praecordium, radiates to the axilla, and is accentuated by expiration.
Aortic stenosis is an ejection systolic murmur heard loudest at the aortic area, radiates to the carotids, and in accentuated by the patient leaning forward in expiration.
Mitral stenosis is a mid-diastolic rumbling murmur heard at the apex and accentuated with the patient leaning on the left side in expiration.
Aortic regurgitation is an early-diastolic murmur heard best at the left sternal edge/tricuspid area, accentuated by the patient leaning forward in expiration.
Aortic stenosis is an ejection systolic murmur heard loudest at the aortic area, radiates to the carotids, and in accentuated by the patient leaning forward in expiration.
Mitral stenosis is a mid-diastolic rumbling murmur heard at the apex and accentuated with the patient leaning on the left side in expiration.
Aortic regurgitation is an early-diastolic murmur heard best at the left sternal edge/tricuspid area, accentuated by the patient leaning forward in expiration.
Here some video that might help you to differentiate between those murmurs
MITRAL REGURGITATION
AORTIC STENOSIS
MITRAL STENOSIS
AORTIC REGURGITATION
- 10:03:00 AM
- 0 Comments


- 11:58:00 PM
- 0 Comments




- 11:56:00 PM
- 0 Comments


- 11:52:00 PM
- 0 Comments


- 11:50:00 PM
- 0 Comments


 |
| SOURCE : MY NOTES FOR USMLE |
Schizophrenia is a serious brain disorder that distorts the way a person thinks, acts, expresses emotions, perceives reality, and relates to others. People with schizophrenia -- the most chronic and disabling of the major mental illnesses -- often have problems functioning in society, at work, at school, and in relationships. Schizophrenia can leave its sufferer frightened and withdrawn. It is a life-long disease that cannot be cured but can be controlled with proper treatment.
Contrary to popular belief, schizophrenia is not a split or multiple
personality. Schizophrenia is a psychosis, a type of mental illness in which a person cannot tell what is real from what is imagined. At times, people with psychotic disorders lose touch with reality. The world may seem like a jumble of confusing thoughts, images, and sounds. The behavior of people with schizophrenia may be very strange and even shocking. A sudden change in personality and behavior, which occurs when schizophrenia sufferers lose touch with reality, is called a psychotic episode.

Who Gets Schizophrenia?
Anyone can get schizophrenia. It is diagnosed all over the world and in all races and cultures. While it can occur at any age, schizophrenia typically first appears in the teenage years or early 20s. The disorder affects men and women equally, although symptoms generally appear earlier in men (in their teens or 20s) than in women (in their 20s or early 30s). Earlier onset of symptoms has been linked to a more severe course of illness. Children over the age of 5 can develop schizophrenia, but it is very rare before adolescence.
At one time, doctors classified schizophrenia based on distinct subtypes:
- Paranoid: Where someone feels he is being persecuted or spied on.
- Disorganized: Where people appear confused and incoherent.
- Catatonic: Where people can be physically immobile or unable to speak.
- Undifferentiated schizophrenia: Asubtype in which no paranoid, disorganized or catatonic features are prominent
- Residual Schizophrenia: In which psychotic symptoms are markedly diminished or no longer present
Scientists think the above distinctions are no longer as accurate or useful as once thought and therefore instead just focus on describing symptoms and their severity.
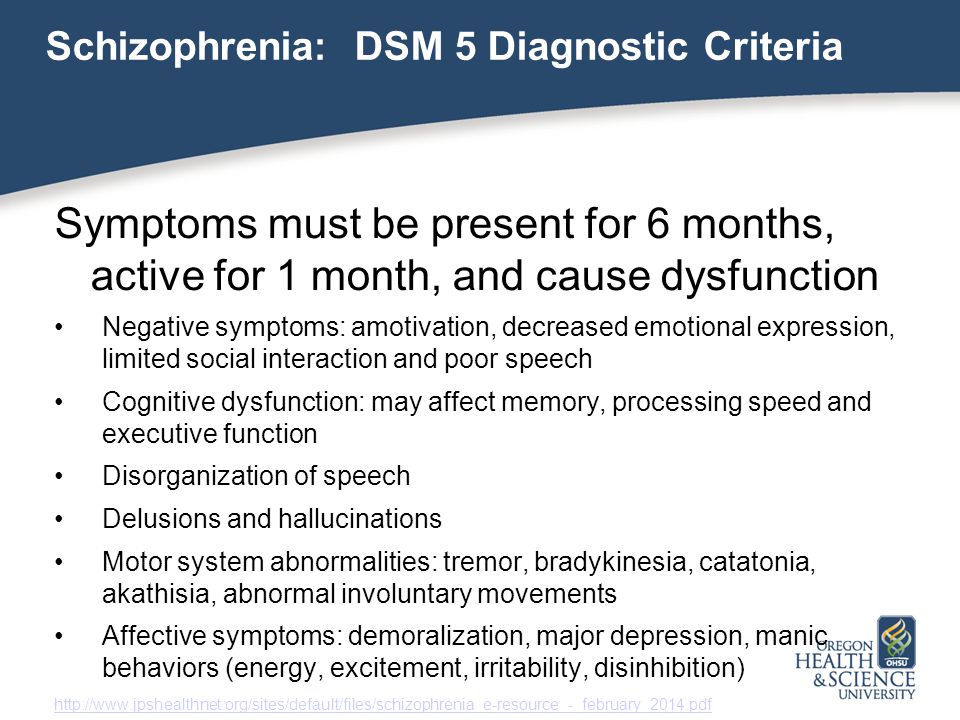
The most common symptoms of schizophrenia can be grouped into several categories including positive symptoms, cognitive symptoms, and negative symptoms.

Positive Symptoms of Schizophrenia
In this case, the word positive does not mean "good." Rather, it refers to obvious symptoms that are exaggerated forms of thinking or behavior that become irrational. These symptoms, which are sometimes referred to as psychotic symptoms, include:
- Delusions: Delusions are strange beliefs that are not based in reality and that the person refuses to give up, even when presented with factual information. For example, the person suffering from delusions may believe that people can hear his or her thoughts, that he or she is God or the devil, or that people are putting thoughts into his or her head or plotting against them.
- Hallucinations: These involve perceiving sensations that aren't real, such as seeing things that aren't there, hearing voices, smelling strange odors, having a "funny" taste in your mouth, and feeling sensations on your skin even though nothing is touching your body. Hearing voices is the most common hallucinationin people with schizophrenia. The voices may comment on the person's behavior, insult the person, or give commands.
- Catatonia (a condition in which the person becomes physically fixed in a single position for a very long time).
Disorganized symptoms of schizophrenia are a type of positive symptom that reflects the person's inability to think clearly and respond appropriately. Examples of disorganized symptoms include:
- Talking in sentences that do not make sense or using nonsense words, making it difficult for the person to communicate or engage in conversation
- Shifting quickly from one thought to the next
- Moving slowly
- Being unable to make decisions
- Writing excessively but without meaning
- Forgetting or losing things
- Repeating movements or gestures, such as pacing or walking in circles
- Having problems making sense of everyday sights, sounds, and feelings
Cognitive Symptoms of Schizophrenia
Cognitive symptoms include:
- Poor executive functioning (the ability to understand information and to use it to make decisions)
- Trouble focusing or paying attention
- Difficulty with working memory (the ability to use information immediately after learning it)

Negative Symptoms of Schizophrenia
In this case, the word negative does not mean "bad," but reflects the absence of certain normal behaviors in people with schizophrenia. Negative symptoms of schizophrenia include:
- Lack of emotion or a very limited range of emotions
- Withdrawal from family, friends, and social activities
- Reduced energy
- Reduced speech
- Lack of motivation
- Loss of pleasure or interest in life
- Poor hygiene and grooming habits
What Causes Schizophrenia?
The exact cause of schizophreniais not yet known. It is known, however, that schizophrenia -- like cancer and diabetes -- is a real illness with a biological basis. It is not the result of bad parenting or personal weakness. Researchers have uncovered a number of factors that appear to play a role in the development of schizophrenia, including:
- Genetics (heredity): Schizophrenia can run in families, which means a greater likelihood to develop schizophrenia may be passed on from parents to their children.
- Brain chemistry and circuits: People with schizophrenia may have abnormal regulation of certain chemicals (neurotransmitters) in the brain, related to specific pathways or "circuits" of nerve cells that affect thinking and behavior. Different brain circuits form networks for communication throughout the brain. Scientists think that problems with how these circuits operate may result from trouble with certain receptors on nerve cells for key neurotransmitters (like glutamate, GABA, or dopamine), or with other cells in the nervous system (called "glia") that provide support to nerve cells within brain circuits. The illness is not believed to be simply a deficiency or "imbalance" of brain chemicals, as was once thought.
- Brain abnormality: Research has found abnormal brain structure and function in people with schizophrenia. However, this type of abnormality doesn't happen in all schizophrenics and can occur in people without the disease.
- Environmental factors: Evidence suggests that certain environmental factors, such as a viral infection, extensive exposure to toxins like marijuana, or highly stressful situations, may trigger schizophrenia in people who have inherited a tendency to develop the disorder. Schizophrenia more often surfaces when the body is undergoing hormonal and physical changes, such as those that occur during the teen and young adult years.
How Do Doctors Diagnose Schizophrenia?
There’s no simple test to find out if someone you love has schizophrenia. It’s a severe mental illness that is very hard to diagnose. It affects the way a person thinks, processes emotions, maintains relationships, and makes decisions.
It’s especially hard to diagnose in teenagers because many of the first signs of schizophrenia in young people, such as bad grades, sleeping too much, or withdrawal from friends, can at first seem like typical problems. But schizophrenia is much more than that.

Is It Schizophrenia?
If you think someone you know may have schizophrenia, reach out to your doctor or psychiatrist. Tell them what you have noticed and ask them what steps you should take, especially if the person isn’t interested in getting help.
The first thing they will want to do is a psychological evaluation and a complete medical exam. This will allow the doctor or specialist to track your loved one’s symptoms over about six months to rule out other possible conditions, such as bipolar disorder, and other possible causes.
The doctor may also want to do a blood test to make sure that alcohol or drug abuse isn’t causing the symptoms. And a test that scans the body and brain, such as an MRI or CT scan, might also help eliminate other problems like a brain tumor.
Making the Diagnosis
To get an official diagnosis of schizophrenia, your loved one has to show at least two of the following symptoms most of the time for a month, and some mental disturbance over six months:
- Delusions (false beliefs that the person won’t give up, even when they get proof that they’re not true)
- Hallucinations (hearing or seeing things that aren’t there)
- Disorganized speech and behavior
- Catatonic or coma-like daze
- Bizarre or hyperactive behavior
Getting the diagnosis as early as possible will improve your loved one’s chances of managing the illness. If he gets the proper care, which will probably include medication and psychotherapy, a kind of talk therapy, he is likely to do better.
SOURCE : WEBMD
SOURCE : WEBMD
- 11:13:00 PM
- 0 Comments







- 5:31:00 PM
- 0 Comments
 |
| credit: pinterest |
B R E A S T . F E E D I N G
 |
| credit: pinterest |
 |
| credit: pinterest |
- 6:26:00 PM
- 0 Comments

Definition of
Gestational Diabetes Mellitus
The WHO has defined
Diabetes Mellitus as either a raised fasting blood glucose level of > 7.8
mmol/L or a level of > 11.0 mmol/L 2 hours following a 75 g oral glucose
load.
Pathogenesis of
Gestational Diabetes Mellitus
Fetal hyperinsulinemia
Effects of Fetal
Hyperinsulinemia
1. Reduced lung
surfactant à
Respiratory Distress Syndrome (RDS)
2. Increased
erythropoiesis can leads to jaundice or hyperviscosity syndrome. Hyperviscosity
syndrome will later develops into necrotizing colitis or renal vein thrombosis.
3. Increased fetal
metabolism which will increases O2 demand. Low O2 supply from the mother can
leads to intrauterine death.
4. Macrosomia à shoulder dystocia
5. Hypoglycaemia
6. Hypertrophic
myocardiopathy
Effects of Diabetes on
Pregnancy
1. Increased
miscarriage rate
2. Increased perinatal
loss due to intrauterine death (IUD)
3. Macrosomic baby
hence is at risk of dystocia
4. Fetal lung
maturation may be delayed; if the fetus was delivered prematurely, the risk of
getting RDS is increased
5. Risk of
preeclampsia
6. Risk of
polyhydramnios
7. Susceptible to
infections; mainly UTI and candida vaginitis
Management of Diabetes
A.
Pre pregnancy
The women who are known
to be diabetic and women who have had gestational diabetes should seek medical
attention before they get pregnant. This consultation offers opportunities in
explaining to them about;
1. The reason for
meticulously maintaining her blood glucose at normal level before conception
2. The need of taking
folic acid to reduce the risk of neural tube defects
This consultation can
also be used as an assessment for the presence of any complication related to
diabetes, such as diabetic retinopathy and nephropathy. Women who are on oral
hypoglycemic drugs should preferably be changed to insulin therapy. We should
check for her glycosylated Hemoglobin, HbA1c that reflects her glucose control
over the previous 10 weeks. High levels of HbA1c are associated with an increased
rate of fetal abnormality.
B. Pregnancy
Euglycemic state
should be maintained; with fasting glucose less than 5.3mmol/L and 2 hour post
prandial blood glucose should be less than 6.7 mmol/L. Blood sugar profile
should be checked before or after each meal; preprandial or postprandial
glucose level and the result should be less than 6 mmol/L or 6.7mmol/L,
respectively. Normal blood glucose level should be maintained with a mixture of
short and medium-acting insulin. Ultrasound scan that was done during the first
12 weeks of pregnancy provides accurate estimation of the period of gestation.
Meanwhile, scanning between 18– 20 weeks of gestation allows exclusion of any
major malformations and around 34 weeks of gestation, it permits assessment of
fetal growth. Regular assessment of fetal growth and wellbeing should be
performed.
C. Timing of Delivery
Delivery at up to 40
weeks of gestation is possible if the sugar control is good. But if there is
inadequate blood glucose control, or the presence of polyhydramnios, fetal
macrosomia or maternal obesity delivery at 38 weeks of gestation is indicated.
Delivery at earlier than 38 weeks is not really indicated to prevent
Respiratory Distress Syndrome in the premature baby.
Management of Labour
The intention is to achieve vaginal delivery.
Labour can be induced by doses of oxytocin. An artificial rupture of membrane
(ARM) should be performed. Blood glucose level needs to be monitored at
frequent intervals; mostly done at 2hourly. The fetus should be monitored
throughout labour and during vaginal delivery shoulder dystocia should be
anticipated. On the other hand, a caesarean section may be performed if there
is significant petal macrosomia or poor fetal status (CTG), or if labour fails
to progress satisfactorily. Uncomplicated diabetes not an indication for
operative delivery.
Follow Up of Women Who
Have Had Gestational Diabetes Mellitus
Follow up is important
as up to 50% of women with Gestational Diabetes Mellitus may develop overt
diabetes; mainly Type II. At the follow up visits, we should encourage her to
follow a diet which is appropriate for a diabetic. She should also be advised
to take these following measures;
1. Avoid becoming
obese
2. Take regular
exercises
3. Avoid cigarette
smoking
4. Checked annually
for hypertension
These women have a 50%
chance of developing Gestational Diabetes Mellitus in the future pregnancy. If
she intend to become pregnant again, testing for hyperglycaemia before
conception or in early pregnancy is recommended.

- 12:34:00 PM
- 0 Comments














