


- 8:28:00 PM
- 0 Comments

Day 1 : The Clinical Long Case in O&G ward, 3 May 2017
I slept at 4 am last night. So tiring and I need to be at hospital by 8 am. Another 1 and half hour. *Sigh*
When I arrive at the labour room, Mdm Wee is waiting for us. Hahaha, I'm so nervous and scared. Remember Prof. Che Anuar ? the one that I told before? Hahaha, I got him as for my long case examiner. Actually, we already knew most of the cases in the hospital that time. Surprisingly the cases that we thought the least probability to come out, were the one that was chose by Dr. Poh for the long case exam. Got patient with multinodular goitre and gestational diabetes during pregnancy. Then one of my friend got monochorionic diamniotic twin with chronic hypertension ! We never had the experiences to palpate the twin. And the twin was one with the cephalic presentation and another one was with breech.
There was also a pregnant lady with asthma. Need to focus on her antenatal care and also the management outline for asthma patient in pregnancy, The pathophysiology of asthma is very important and it was taught to us so many time in our previous posting.

I'm getting nervous and more nervous. I am the second last candidate for the long case. I'm the 21 of 23 students. hahaha, I have waited from 8 am till 11.10 am for my turn to examine the patient.
What happened was, we shared patients for our long case exam. So, the patient has been examined by another student before me. The patient that time was so anxious and tired. She was in pain as she claimed she has been administered with progestin vaginally to induce labour that morning.
She refused to continue the examination, and I'm so done. Terkebil kebil aku berdiri tepi cardiac table tu tengok dia strongly refuse to continue the session. Then I tried to persuade her. She said she want to take bath. So yeaaaa, tinggallah aku kat situ sadly, alone and jotted down all important things from her pink book (Antenatal Check Up Book).
Luckily Dr. Poh ada and pujuk patient to cooperate. Thank you Dr. Poh !! I managed to finish my history taking and physical examinations. My patient was in pain so I couldn't perform any examination in front of Prof Anuar, but luckily I had examine her before that. Now I'm afraid of how he will evaluate me without physical examination. My history taking alone is not sufficient. I just hope he will consider and let me pass this time. I really hope so.



When I arrive at the labour room, Mdm Wee is waiting for us. Hahaha, I'm so nervous and scared. Remember Prof. Che Anuar ? the one that I told before? Hahaha, I got him as for my long case examiner. Actually, we already knew most of the cases in the hospital that time. Surprisingly the cases that we thought the least probability to come out, were the one that was chose by Dr. Poh for the long case exam. Got patient with multinodular goitre and gestational diabetes during pregnancy. Then one of my friend got monochorionic diamniotic twin with chronic hypertension ! We never had the experiences to palpate the twin. And the twin was one with the cephalic presentation and another one was with breech.
There was also a pregnant lady with asthma. Need to focus on her antenatal care and also the management outline for asthma patient in pregnancy, The pathophysiology of asthma is very important and it was taught to us so many time in our previous posting.
I'm getting nervous and more nervous. I am the second last candidate for the long case. I'm the 21 of 23 students. hahaha, I have waited from 8 am till 11.10 am for my turn to examine the patient.
What happened was, we shared patients for our long case exam. So, the patient has been examined by another student before me. The patient that time was so anxious and tired. She was in pain as she claimed she has been administered with progestin vaginally to induce labour that morning.
She refused to continue the examination, and I'm so done. Terkebil kebil aku berdiri tepi cardiac table tu tengok dia strongly refuse to continue the session. Then I tried to persuade her. She said she want to take bath. So yeaaaa, tinggallah aku kat situ sadly, alone and jotted down all important things from her pink book (Antenatal Check Up Book).
Luckily Dr. Poh ada and pujuk patient to cooperate. Thank you Dr. Poh !! I managed to finish my history taking and physical examinations. My patient was in pain so I couldn't perform any examination in front of Prof Anuar, but luckily I had examine her before that. Now I'm afraid of how he will evaluate me without physical examination. My history taking alone is not sufficient. I just hope he will consider and let me pass this time. I really hope so.
HISTORY TAKING
My patient is Puan X, age 35 years old, G3P2 and currently at 37 weeks of POA. Her LNMP not stated in the pink book and patient couldn't recall the exact date. Her EDD, given by the ultrasound is on 20 May 2017.
She was admitted to the ward on 29 April 2017 due to presentation of blood mixed with mucous.
Patient claimed that she notice presence of show when she was going to take bath in the morning. She noticed the show soaked half of her panty and she decide to come to hospital after that. Patient also said that there was decrease in fetal movement.
Otherwise, there was;
- no abdominal pain
- no leaking
- no fever
- no UTI symptoms
Upon admission, her os dilatation was 2 cm. She was asked to rest and monitored closely in ward. She was not in pad chart monitoring. 2 days later she noticed presence of blood spotting mixed with mucous again, soaked her panty. The doctor in charged did vaginal examination on her and the cervical dilatation that time was still 2 cm. The next day, she claimed to have abdominal pain with increase frequency and intensity. It was increasing in frequency in 10 minutes for 20-30 seconds. It then stopped for 2 minutes and then start again. The pain subsided at night. The next morning, doctor did vaginal examination again and cervical os was 3 cm dilated. According to patient, she was given drug vaginally to induce her labour because of decrease in fetal movement.
Antenatal History
She did not noticed when she missed her period. She experienced mild vomiting 2 times/day for 2 months and thought it was only one of her gastritis symptoms. She went to Klinik Kesihatan Bawah Tanjung and did urine pregnancy test and the result was positive.
Her booking date was on 9 October 2016 at Klinik Kesihatan Bawah Tanjung. Her height and weight upon booking were 157 cm and 59 kg respectively, and her BMI was 23.9 kg/m2
Series of investigations were done upon booking. Her haemoglobin level was 12.0 g/dL, her blood pressure was 110/70 mmHg and her pulse rate was 90 beats/min. The uterus was not palpable yet that time. Because of unable to obtain her LNMP, first ultrasound was done upon booking to access gestational age. It was 7 weeks and 5 days of gestation, revealed present of fetal heart.
Her blood group is O rhesus positive. VRDL and HIV screening test were non reactive.
Her latest ultrasound was on 13 February 2017 at 26 weeks of gestation revealed viable, singleton fetus with cephalic presentation. Parameters were corresponding to the gestational age.
BPD - 7.05 cm
AC - 21.58 cm
FL - 4.78 cm
She has completed her anti toxoid tetanus (ATT) immunisation, 2 doses at 20 weeks of POA on 23 April 2016. Oral Glucose Tolerance Test was done on 23 April 2017, at 36 weeks of gestation at KK Bawah Tanjung. and the result was normal. She had experience mild pregnancy symptoms such as nausea, vomiting and lethargic during her first trimester (1-12 weeks).
Gynaecological History
She attained menarche at age of 13 years old, with regular cycle of 28-30 days interval. Bleeding duration was normally 6-7 days, with peak flow on 1st and 2nd day of menses.
Otherwise,
- no dysmenorrhea
- no intermenstrual bleeding
- no post coital bleeding
Obstetric History
She was blessed with two children. Both were delivered normally via spontaneous vaginal delivery at term, ranging birth weight of 2.7-2.8 kg. Both are healthy girls. The first child was born in 2003 and the second child was born in 2010. The was 7 years of gap spacing.
Contraceptive History
Patient did not practice any contraceptive method.
Past Medical and Surgical History
Nil
Drugs History
She only take the vitamins supplement for pregnancy that was prescribed by the klinik kesihatan.
Family History
Her mother was diagnosed with heart disease. Her father has passed away in 2001 due to intestunal cancer. Other family member are healthy.
Nutritional History
She take 3 major meals per day of normal balanced diet with snacks in between.
Social History
She work as an assistant in a shop. Her husband's age is 39 years old, working as sellers. He is a smoker.
In summary, my patient is a 35 years old lady, G3P2 at 37 weeks of period of amenorrhea came due to show presentation. Patient is in labour.
I'm so done with O&G. For sure this is not my field ! What to do?
Questions that been asked to me by Prof Anuar were:
- What are the cause of decrease fetal movement? - engagement of the head to pelvis, oligohyroamnious, mass in the uterus.
- What investigations I would want to do in this patient? Hb evaluation, CTG, Ultrasound
- Why is the purpose of CTG? - to access fetal well being, to access fetal hypoxia and fetal acidosis.
- Fetal hypoxia because of somatic or neurological hypoxia? Somatic hypoxia
- Which component of CTG reflect the fetal autonomic nervous system? The baseline variability (beat to beat varies).
- Autonomic nervous system was controlled by what? Baroreceptor and chemoreceptor.
- How to diagnose fetal acidotic, what test should be done? Arterial blood gas sample from fetal scalp blood testing.
- The management? Allow labour.
Day 1 : The Written Examination in college, 4 May 2017
Well. Conclusion for today is everything is suck. The MEQ and OSCE were so hard to answer as we were prepared for the diseases in pregnancy or the abnormal labour. Instead they gave us the mechanism of normal labour. Hahahaha, I've read it but I could only remember few steps that involved in the mechanism. I'm doomed. I just hope I pass this posting. That's all. Gotta qada' my sleep now.
- 9:57:00 PM
- 0 Comments

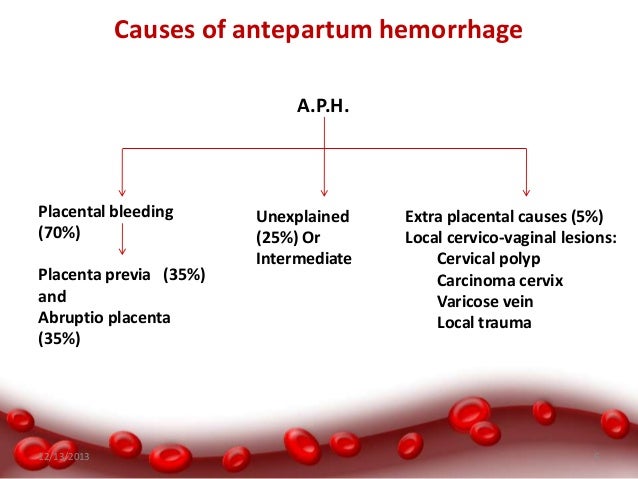
Antepartum haemorrhage (APH) is defined as bleeding from or in to the genital tract, occurring from 24+0
weeks of pregnancy and prior to the birth of the baby. The most important causes of APH are placenta praevia
and placental abruption, although these are not the most common. APH complicates 3–5% of pregnancies and
is a leading cause of perinatal and maternal mortality worldwide. Up to one-fifth of very preterm babies are
born in association with APH, and the known association of APH with cerebral palsy can be explained by
preterm delivery.
Obstetric haemorrhage remains one of the major causes of maternal death in developing countries and is the cause of up to 50% of the estimated 500 000 maternal deaths that occur globally each year. Obstetric haemorrhage encompasses both antepartum and postpartum bleeding.

There are no consistent definitions of the severity of APH. It is recognised that the amount of blood lost is often underestimated and that the amount of blood coming from the introitus may not represent the total blood lost (for example in a concealed placental abruption). It is important therefore, when estimating the blood loss, to assess for signs of clinical shock. The presence of fetal compromise or fetal demise is an important indicator of volume depletion.
For the purposes of this guideline, the following definitions have been used:
Recurrent APH is the term used when there are episodes of APH on more than one occasion
Obstetric haemorrhage remains one of the major causes of maternal death in developing countries and is the cause of up to 50% of the estimated 500 000 maternal deaths that occur globally each year. Obstetric haemorrhage encompasses both antepartum and postpartum bleeding.
There are no consistent definitions of the severity of APH. It is recognised that the amount of blood lost is often underestimated and that the amount of blood coming from the introitus may not represent the total blood lost (for example in a concealed placental abruption). It is important therefore, when estimating the blood loss, to assess for signs of clinical shock. The presence of fetal compromise or fetal demise is an important indicator of volume depletion.
For the purposes of this guideline, the following definitions have been used:
- Spotting – staining, streaking or blood spotting noted on underwear or sanitary protection Minor haemorrhage – blood loss less than 50 ml that has settled
- Major haemorrhage – blood loss of 50–1000 ml, with no signs of clinical shock
- Massive haemorrhage – blood loss greater than 1000 ml and/or signs of clinical shock
Recurrent APH is the term used when there are episodes of APH on more than one occasion
What is the role of clinical assessment in women presenting with APH?
The role of clinical assessment in women presenting with APH is first to establish whether urgent
intervention is required to manage maternal or fetal compromise. The process of triage includes history
taking to assess coexisting symptoms such as pain, an assessment of the extent of vaginal bleeding,
the cardiovascular condition of the mother, and an assessment of fetal well being.
Women presenting with a major or massive haemorrhage that is persisting or if the woman is unable to
provide a history due to a compromised clinical state, an acute appraisal of maternal well being should be
performed and resuscitation started immediately. The mother is the priority in these situations and should be
stabilised prior to establishing the fetal condition.
If there is no maternal compromise a full history should be taken.
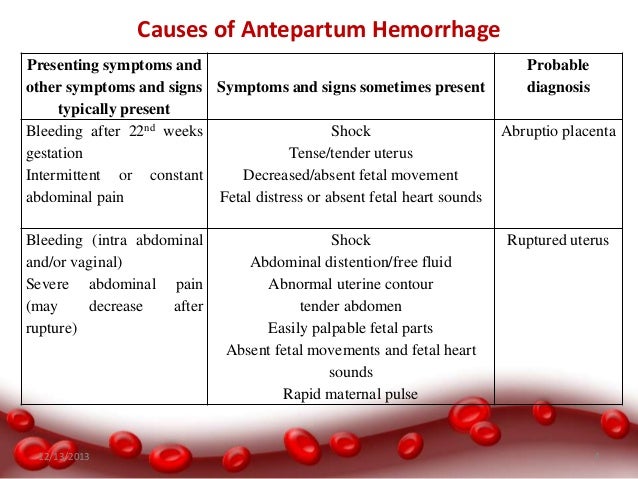
● The clinical history should determine whether there is pain associated with the haemorrhage. Placental abruption should be considered when the pain is continuous. Labour should be considered if the
pain is intermittent.
● Risk factors for abruption and placenta praevia should be identified.
● The woman should be asked about her awareness of fetal movements and attempts should be made to
auscultate the fetal heart.
● If the APH is associated with spontaneous or iatrogenic rupture of the fetal membranes, bleeding from a
ruptured vasa praevia should be considered.
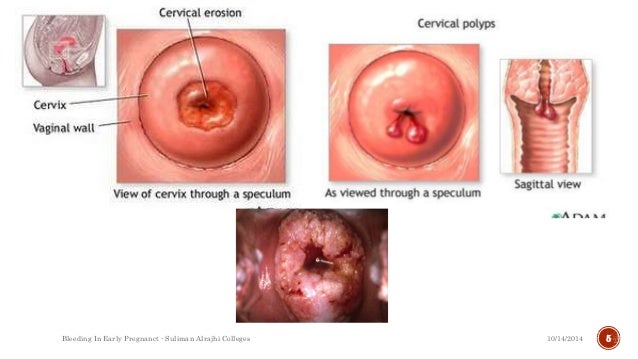
● Previous cervical smear history may be useful in order to assess the possibility of a neoplastic lesion of the
cervix as the cause of bleeding.
The presentation of cervical cancer in pregnancy depends on the stage at
diagnosis and lesion size; most women with International Federation of Gynecology and Obstetrics (FIGO)
stage I cancer are asymptomatic; symptomatic pregnant women usually present with APH (mostly postcoital)
or vaginal discharge.
In a Swedish population study, the incidence of cervical cancer was 7.5 cases per
100 000 deliveries; in over half of these cases, the women had an abnormal cervical smear history.
Examination of the woman should be performed to assess the amount and cause of APH.
The basic principles of resuscitation should be adhered to in all women presenting with collapse or major
haemorrhage.
The primary survey should follow the structured approach of airway (A),
breathing (B) and circulation (C). Following initial assessment and commencement of resuscitation, causes for
haemorrhage or collapse should be sought.
All women presenting with APH should have their pulse and blood pressure recorded.
Abdominal palpation
The woman should be assessed for tenderness or signs of an acute abdomen. The tense or ‘woody’ feel to the
uterus on abdominal palpation indicates a significant abruption. Abdominal palpation may also reveal uterine
contractions. A soft, non-tender uterus may suggest a lower genital tract cause or bleeding from placenta or
vasa praevia.
A speculum examination can be useful to identify cervical dilatation or visualise a lower genital
tract cause for the APH. In a prospective observational study of 564 women presenting with APH,
521 (92.4%) underwent an admission speculum examination; 389 women (69%) had a normal
cervix, 120 (21%) had cervical ectropion and 12 (2%) had a dilated cervix. If the woman presents with a clinically suspicious cervix she should be referred for colposcopic
evaluation
Digital vaginal examination
If placenta praevia is a possible diagnosis (for example, a previous scan shows a low placenta, there is a high
presenting part on abdominal examination or the bleed has been painless), digital vaginal examination should
not be performed until an ultrasound has excluded placenta praevia. Digital vaginal examination can provide
information on cervical dilatation if APH is associated with pain or uterine activity.
What investigations should be performed in women presenting with APH?
Maternal investigations
Investigations should be performed to assess the extent and physiological consequences of the APH.
The maternal investigations performed will depend on the amount of bleeding.
The Kleihauer test should be performed in rhesus D (RhD)-negative women to quantify fetomaternal
haemorrhage (FMH) in order to gauge the dose of anti-D immunoglobulin (anti-D Ig) required.
The Kleihauer test is not a sensitive test for diagnosing abruption.
Ultrasound can be used to diagnose placenta praevia but does not exclude abruption. Placental abruption is a clinical diagnosis and there are no sensitive or reliable diagnostic tests
available. Ultrasound has limited sensitivity in the identification of retroplacental haemorrhage.
Blood tests
In cases of major or massive haemorrhage, blood should be analysed for full blood count and coagulation
screen and 4 units of blood cross-matched. Urea, electrolytes and liver function tests should be assayed. The
initial haemoglobin may not reflect the amount of blood lost and therefore clinical judgement should be used
when initiating and calculating the blood transfusion required. In such circumstances a point of care test
(‘bedside test’) to assess haemoglobin may be useful.
The platelet count, if low, may indicate a consumptive
process seen in relation to significant abruption; this may be associated with a coagulopathy.
In minor haemorrhage, a full blood count and group and save should be performed.
A coagulation screen is
not indicated unless the platelet count is abnormal.
In all women who are RhD-negative, a Kleihauer test should be performed to quantify FMH to
gauge the dose of anti-D Ig required.
The Kleihauer test is not a sensitive test for diagnosing placental abruption.
Ultrasound scan
Women presenting with APH should have an ultrasound scan performed to confirm or exclude placenta
praevia if the placental site is not already known. Ultrasound scanning is well established in determining
placental location and in the diagnosis of placenta praevia.
The sensitivity of ultrasound for the detection of retroplacental clot (abruption) is poor. Glantz and
colleagues reported the sensitivity, specificity, and positive and negative predictive values of
ultrasonography for placental abruption to be 24%, 96%, 88% and 53% respectively. Thus,
ultrasonography will fail to detect three-quarters of cases of abruption. However, when the
ultrasound suggests an abruption, the likelihood that there is an abruption is high.
Fetal investigation
An assessment of the fetal heart rate should be performed, usually with a cardiotocograph (CTG) in
women presenting with APH once the mother is stable or resuscitation has commenced, to aid decision
making on the mode of delivery.
Whenever possible, CTG monitoring should be performed where knowledge of fetal condition will
influence the timing and mode of delivery.
Ultrasound should be carried out to establish fetal heart pulsation if fetal viability cannot be detected
using external auscultation.
APH, particularly major haemorrhage and that associated with placental abruption, can result in fetal
hypoxia and abnormalities of the fetal heart rate pattern. If the fetal heart rate cannot be heard on
auscultation, then an ultrasound scan should be performed to exclude an intrauterine fetal death.
Ultrasound imaging can be technically difficult, particularly in the presence of maternal obesity,
abdominal scars and oligohydramnios, but views can often be augmented with colour Doppler.
Guidance directly relevant to monitoring the fetal heart rate at the extreme of viability can be
reasonably extrapolated from advice on the management of women in extremely preterm labour
(less than 26+0 weeks) from the British Association of Perinatal Medicine.
The results of this working
group suggest ‘If active obstetric intervention in the interests of the fetus is not planned, for example
at gestations less than 26+0 weeks, continuous monitoring of the fetal heart rate is not advised. There is a lack of published evidence regarding the role and usefulness of fetal heart-rate monitoring in
women presenting with APH. In one study, the fetal heart-rate pattern (CTG) was abnormal in 69% of women
presenting with placental abruption. Whilst conservative (expectant) management appears to be safe in
preterm pregnancies with placental abruption and a normal CTG, an abnormal CTG is associated with poor
fetal outcome and delivery should be expedited to save the fetus.
Clinical judgement is required in these
circumstances since women presenting with bleeding that may indicate a catastrophic event such as
placental abruption, constitute a group where the fetus is more likely to be exposed to severe hypoxia and
acidaemia. In such circumstances, the CTG can reasonably be expected to be informative.
Labour and delivery
When should women with APH be delivered and what mode of delivery should be employed in women
whose pregnancies have been complicated by APH?
If fetal death is diagnosed, vaginal birth is the recommended mode of delivery for most women
(provided the maternal condition is satisfactory), but caesarean birth will need to be considered for
some.
If the fetus is compromised, a caesarean section is the appropriate method of delivery with concurrent
resuscitation of the mother.
Women with APH and associated maternal and/or fetal compromise are required to be delivered
immediately.
The optimum timing of delivery of women presenting with unexplained APH and no associated maternal
and/or fetal compromise is not established.
A senior obstetrician should be involved in determining the
timing and mode of birth of these women.
In women with APH secondary to placenta praevia, intrapartum management is described in Green-top
Guideline No. 27
APH associated with maternal or fetal compromise is an obstetric emergency. Management should include
maternal resuscitation and delivery of the fetus to control the bleeding. Delivery in this situation will usually be by caesarean section, unless the woman is in established labour. Similarly, if there is
evidence of fetal distress, resuscitation of the mother should commence and arrangements made to deliver
the baby by caesarean section once the woman is stabilised.




Definition
- Placenta previa is a condition wherein the placenta of a pregnant woman is implanted abnormally in the uterus. It accounts for the most incidents of bleeding in the third trimester of pregnancy.
Pathophysiology
- The placenta implants on the lower part of the uterus.
- The lower uterine segment separates from the upper segment as the cervix starts to dilate.
- The placenta is unable to stretch and accommodate the shape of the cervix, resulting in bleeding.


- Low lying placenta. The placenta implants in the lower portion instead of the upper portion of the uterus.
- Marginal implantation. The placenta’s edge is nearing the cervical os.
- Partial placenta previa. A portion of the cervical os is already covered by the placenta.
- Total placenta previa. The placenta occludes the entire cervical os.



Signs and Symptoms
The following signs and symptoms for placenta previa must be detected immediately by the health care providers to avoid risking the life of the fetus.
- Bright red bleeding. When the placenta is unable to stretch to accommodate the shape of the cervix, bleeding will occur suddenly that could frighten the woman.
- Painless. Bleeding in placenta previa is not painless and may also stop as abruptly as it had begun.
Diagnostic Tests
To diagnose placenta previa, the patient must undergo the following diagnostic procedure.
- Ultrasound. Early detection of placenta previa is always possible through ultrasonography. It is the most common and initial diagnostic test that could confirm the diagnosis.
Medical Management
Medical interventions are necessary to ensure that the safety of both mother and fetus are still intact.
- Intravenous therapy. This would be prescribed by the physician to replace the blood that was lost during bleeding.
- Avoid vaginal examinations. This may initiate hemorrhage that is fatal for both the mother and the baby.
- Attach external monitoring equipment. To monitor the uterine contractions and record fetal heart sounds, an external equipment is preferred than the internal monitoring equipment.
Surgical Management
Surgical interventions are carried out once the condition of both the mother and the fetus has reached a critical stage and their lives are exposed to undeniable danger.
- Cesarean delivery. Although the best way to deliver a baby is through normal delivery, if the placenta has obstructed more than 30% of the cervical os it would be hard for the fetus to get past the placenta through normal delivery. Cesarean birth is then recommended by the physician.
Nursing Assessment
- Assess baseline vital signs especially the blood pressure. The physician would order monitoring of the blood pressure every 5-15 minutes.
- Assess fetal heart sounds to monitor the wellbeing of the fetus.
- Monitor uterine contractions to establish the progress of labor of the mother.
- Weigh perineal pads used during bleeding to calculate the amount of blood lost.
- Assist the woman in a side lying position when bleeding occurs.
Nursing Interventions
- Assess fetal heart sounds so the mother would be aware of the health of her baby.
- Allow the mother to vent out her feelings to lessen her emotional stress.
- Assess any bleeding or spotting that might occur to give adequate measures.
- Answer the mother’s questions honestly to establish a trusting environment.
- Include the mother in the planning of the care plan for both the mother and the baby.
- 1:49:00 AM
- 0 Comments
Bleeding In First Trimester Of Pregnancy
Vaginal bleeding during pregnancy first trimester can be caused by various factors. Nearly 20 to 30% of pregnancies will be affected with bleeding during this phase.
1. Ectopic Pregnancy:
In an ectopic pregnancy, the fertilized egg implants outside the uterus, that is usually in the fallopian tube. You will usually notice cramping and a sharp pain in the lower abdominal region accompanied by dizziness, weakness and nausea. It can be life threatening to mother and requires immediate medical attention. Statistically, only 3% of pregnancies experience it.
Signs of Ectopic Pregnancies:
- Cramping pain felt low in the stomach (usually stronger than menstrual cramps)
- Sharp pain in the abdominal area
- Low levels of hCG
- Vaginal bleeding
Women are at a higher risk if they have had:
- An infection in the tubes
- A previous ectopic pregnancy
- Previous pelvic surgery
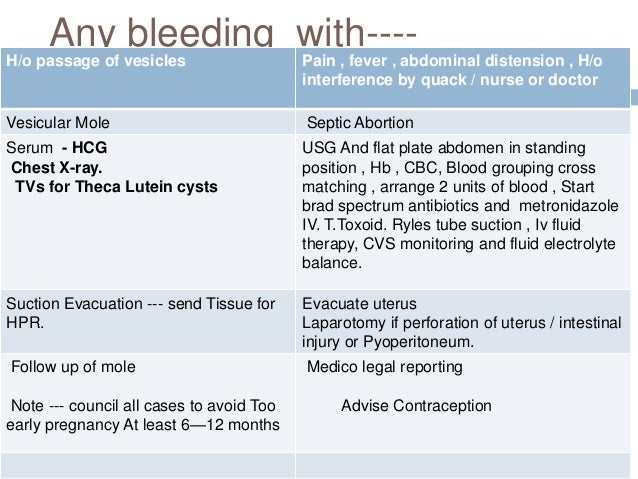
2. Molar Pregnancy:
Molar pregnancy is a rare condition that results when the placenta becomes a cystic mass from a malformed embryo. This is a type of tumor that occurs because of pregnancy hormones and is not life threatening at all. It happens within a few weeks of conception. In some cases, it can turn out to be abnormal and can spread throughout the body, the condition being diagnosed as gestational trophoblastic disease. You can observe vaginal bleeding within few weeks of conception if you happen to suffer from molar pregnancy.
Signs of a Molar Pregnancy:
- Vaginal bleeding
- Blood tests reveal unusually high hCG levels
- Absent fetal heart tones
- Grape-like clusters are seen in the uterus by an ultrasound
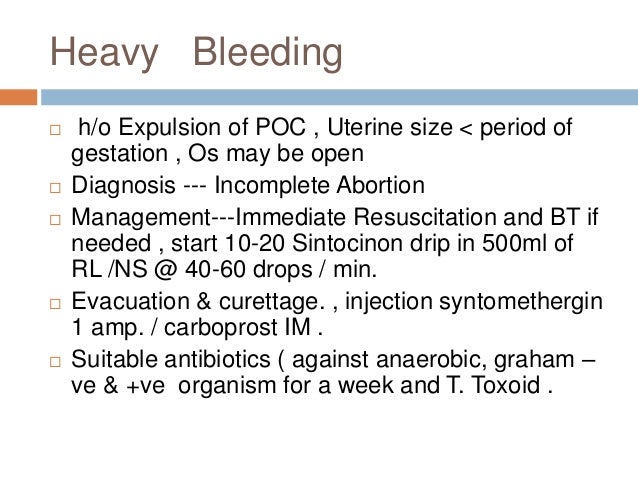
3. Miscarriage:
One of the major concerns with bleeding during first trimester of pregnancy is that it can be a miscarriage as well. It is common to occur during the initial 12 weeks of pregnancy. If bleeding accompanies symptoms like cramping, lower abdominal pain and passage of tissue through the vagina, then there is a higher chance of miscarrying the baby. About 50% pregnant women who experience the symptoms along with vaginal bleeding, miscarry a baby.
Bleeding In Second And Third Trimesters Of Pregnancy
The common cause of bleeding during late pregnancy is due to placenta problems. Also, abnormal cervix or vagina can cause bleeding.
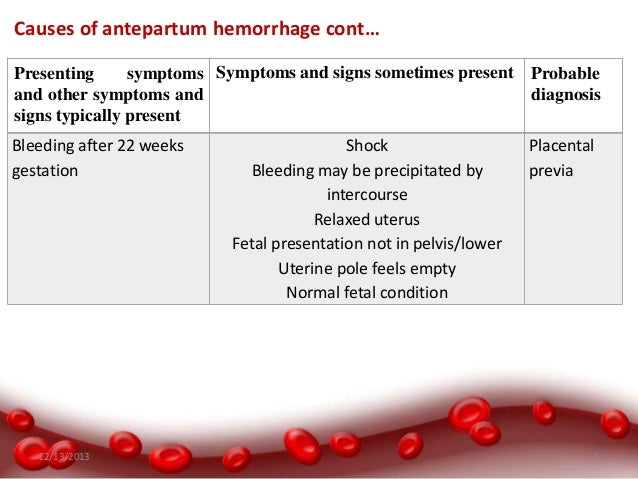
4. Placenta Previa:
This is the most common cause of bleeding during late pregnancy. In this condition, the placenta that usually connects the fetus to the womb will cover a part of the cervical opening. As a result, bleeding takes place. Later in pregnancy, the cervix becomes thin and dilates to prepare for labor. At this stage, the placenta stretches and ruptures causing heavy bleeding. The risk factors for this placenta previa condition include prior placenta previa, multiple pregnancies and prior cesarean delivery.
5. Placenta Abruption:
This condition occurs in the second half of pregnancy or the third trimester. It is an early separation of placenta from the uterus and it leads to blood collection in the region between the placenta and uterus. It is accompanied by cramps, pains in the abdominal region, tenderness in the uterus and back pain. If the separation is too little, it is not lethal for the baby. But, it will pose severe risks if the separation is large. The risk factors for this cause of vaginal bleeding include trauma, hypertension, usage of tobacco, cocaine and prior placenta abruption.
6. Uterine Rupture:
In rare conditions there will be an abnormal splitting of the uterus due to a scar from a prior C-section. It makes the fetus expel into the abdomen that can be quite dangerous for both the baby and the mother. The uterine rupture can occur before or during the labor time. There are certain other risk factors that include trauma, multiple pregnancies, using excess amounts of oxytocin medicine (strengthens contractions) and deliveries through forceps.
7. Fetal Vesssel Rupture:
The developing blood vessels of the fetus may cross the opening of the birth canal. These are known to be vasa previa and can be lethal to the baby as blood vessels can tear open and bleed severely. This condition is also accompanied by abnormal fetal heart rate. It is a very rare condition that happens in 1 out of 5000 pregnancies.
8. Pre-term Labor:
If the delivery time falls between week 20 to week 37, it is considered a pre-term labor. It is accompanied by cramping, regular contractions, built-in pelvic pressure and back pain. A few days before your body prepares for labor, you will pass your mucus plug where bleeding starts. This is termed as a bloody show that requires an immediate contact with your health care provider.
Signs of Preterm Labor include these symptoms that occur before the 37th week of pregnancy:
- Vaginal discharge (watery, mucus, or bloody)
- Pelvic or lower abdominal pressure
- Low, dull backache
- Stomach cramps, with or without diarrhea
- Regular contractions or uterine tightening
Some other causes of bleeding in late pregnancy include:
- Injury to vagina or cervical region
- Cancer
- Polyps
- Varicose veins (abnormal veins with full of twists and turns)
HOW TO DIAGNOSE
Lab Test
Full blood count
Urine Pregnancy Test
Serum b-hCG level
Imaging
Ultrasound
Chest X ray - in case of Molar Pregnancy
Reference
- 1:38:00 PM
- 0 Comments

Topic : Postpartum Care by Association of Professors of Gynecology and Obstetrics (APGO)
Postpartum Maternal Physical Assessment Summary- BUBBLE HE
Breasts:
- inspect: size, symmetry, shape of breast and nipples taking note of erection, flatness, redness, bruising, open wounds, presence of mastitis and colostrum
- palpate: fullness, soft or engorged, firmness and lumps
- pain assessment
Uterus (Fundus):
- palpate: firmness/bogginess, location of the fundus in relation to the abdomen, determine the location of the fundus in relation to the belly button to determine amount of fundal involution
- inspect incision site
- check policy: in some organizations, they may not assess fundal involution by palpation due to fear of dehiscence
Bladder:
- void amount (~30ml/hr)
- assess for distention, incontinence, urinary retention, urinary infection especially if the patient had a foley catheter
Bowel:
- last bowel movement/flatus
- assess for distention, abdominal pain
Lochia:
- amount, color, odour
- assess for postpartum hemorrhage


- Persistent red lochia suggested delay involution that is usually associated with infections or retained piece of placenta tissue.
- Offensive lochia, which may be accompanied by pyrexia and a tender uterus, suggests infections and should be treated with broad spectrum antibiotics.
- Retained placental tissue is associated with increased red blood cell loss and blood clots, and this may be suspected if the placenta and membranes were incomplete at delivery. Management includes uses of antibiotics and evacuation of retained products under regional or general anaesthesia.
Episiotomy
- level of laceration
- number of stitches, redness, edema, bruisin, discharge, approximation of wound edges
- assess perineal area
Homan’s Sign-for DVT
- assess for pain with dorsiflexion
- check policy: this is sometimes not done in organizations
Emotional State:
- assess for signs and symptoms of postpartum depression and infant-maternal bonding
At my postpartum placement, one of the nurses gave us a very helpful handout on what to look for specifically in cesarean and vaginal deliveries postpartum. Again, the Disclaimer is that these were tips she found useful in assessing her patients, do not use this information to guide your practice, checking college standards and organizational regulations is imperative to good practice.
Vaginal Birth Assessment
- VS: on admission; 2 hrs post 1st set of VS; 24hr postpartum or qshift; within 2hr of d/c
- Urine Output: d/c foley when patient is walking; delay foley removal if there is swelling in labia
- IV: d/c when patient is stable and no signs of postpartum hemorrhage
Cesarean Assessment
- VS: on admission; 1hr post 1st set of vitals; q4hrs for the next 48 hrs; qshift until d/c; within 2hrs of d/c
- Urine Output: d/c foley catheter 12 hrs post opt unless ordered; output for first 2 voids should match ~30ml/hr; if no void within 6-8 hrs post foley removal then do I/O catheter
- IV: assess for complications such as infiltration, fluid overload; d/c 24hrs or when stable VS
Neonatal Physical Assessment
- Check: GBS, Bloodtype, HepB, HIV and Rubella status of mother and baby
- VS: on admission; qshift (if GBS+ive then q4h)
- Head to Toe: on admission; qshift; the mother is a great resource wen you are doing vital assessments or when you are getting blood samples for the heel prick. Have the mother hold the baby skin-skin or breast feed the baby when you assess, they cry less and will make the assessment go faster.
- Blood Work: GBS+ive babies need cbc and blood culture 4hrs after birth; bilirubine and newborn screen with heel prick is done after 24hrs for Vaginal births and 48hrs for Cesarean sections
- Breastfeeding: skin-skin as much as possible; breask feed 12-3 hrs or when baby shows feeding cues.
Credit: Nurse Student Opinion
- 7:53:00 PM
- 0 Comments














