


- 6:44:00 PM
- 0 Comments


" 'Doctors' has aired 10 episodes of its 20 total so far. By this point, we’ve been exposed enough to our characters to become invested in their stories. As this show has progressed, I am constantly being impressed by the deft way it has captured the relationships between different individuals. The show has done a fantastic job showing raw human emotions while pairing it with a dash of sweet romance.The beautiful cinematography and the sprinkles of narration by Yoo Hye Jung have really made this drama a joy to watch. Although I was concerned about the teacher-student relationship narrative, I am starting to understand perhaps the story is meant show the growth a of mentor-mentee relationship to that of lovers. This topic, which seems taboo, has been handled with care and a captivating plot." - Soompi
Profile
- Drama: Doctors
- Revised romanization: Dakteoseu
- Hangul: 닥터스
- Director: Oh Choong-Hwan
- Writer: Ha Myung-Hee
- Network: SBS
- Episodes: 20
- Release Date: June 20 - August 23, 2016
- Runtime: Monday & Tuesday 22:00
- Language: Korean
- Country: South Korea

Plot
A drama about the realism in the relationship between doctors and patients and the social prejudice of educational background and origin. Yoo Hye jung (Park Shin Hye) was a tough bully in school with a prickly personality and always goes wayward. She had many scars from her childhood and through self-preservation, Hye Jung keeps her heart shut away from other people. However, she changes after meeting her mentor Hong Ji Hong (Kim Rae Won) who plays a key role in transforming her life from a helpless gangster to a compassionate doctor.DOCTORS


- 8:59:00 PM
- 0 Comments


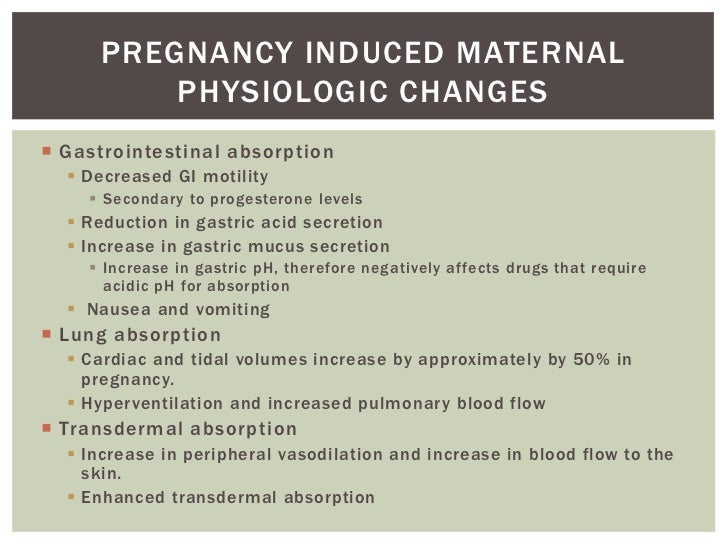
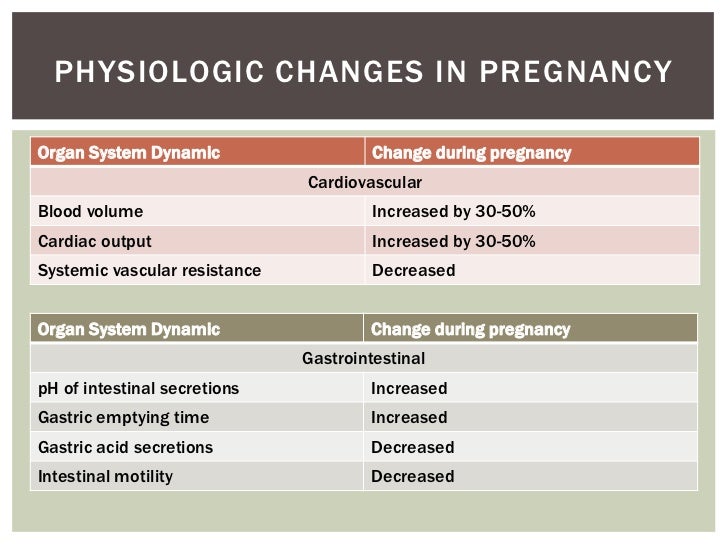
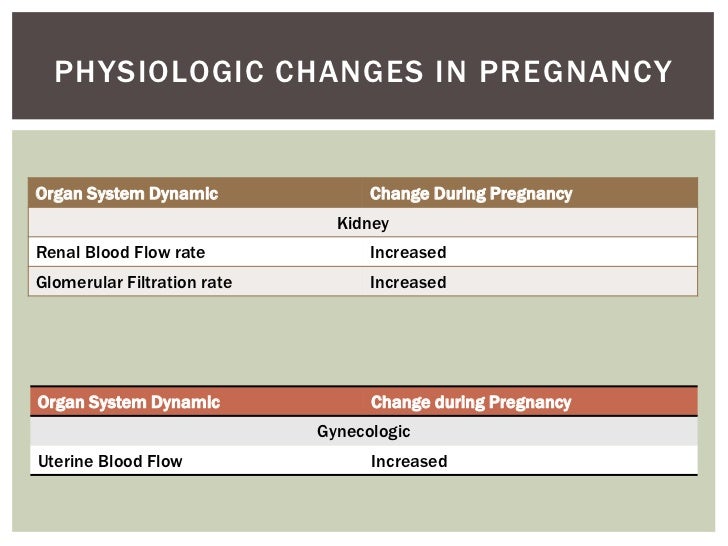
So what happen when you're pregnant?



- 8:32:00 PM
- 0 Comments

So sambil makan popcorns and drinks my cappuccino, mannn this movie is really good. I'm a medical student so I got excited when it involved forensic kinda movie and etc. But, this mysterious body sure is scary as so many weird paranormal thingy happened after they cut open the chest. So yeaaaaa !

T H E . A U T O P S Y . O F . J A N E . D O E
The Autopsy of Jane Doe is a 2016 American supernatural horror film directed by André Øvredal. It stars Emile Hirsch and Brian Cox as father-and-son coroners who experience supernatural phenomena while examining the body of an unidentified woman (played by Olwen Kelly). It premiered at the Toronto International Film Festival on September 9, 2016, and was released on December 21. It is Øvredal's first English-language film.

PLOT :
An unidentified corpse of a woman is found half-buried in the basement of a house where a bloody and bizarre homicide has occurred. One of the police officers concludes that there are no signs of forced entry and the victims seemed to be trying to escape the house instead.

Small-town coroner Tommy Tilden and his son Austin, a medical technician who assists him, have just finished the autopsy of a burned corpse when Austin's girlfriend, Emma, arrives and gets curious about the bodies in the morgue.The sheriff arrives with the mysterious body and tells Tommy that he needs the cause of death (COD) by morning. Austin decides to help his dad instead of going to the theater with Emma, but asks her to come back later. Since no one knows the body's identity and its fingerprints are not on police records, they refer to her as Jane Doe.


External examination of the corpse
- no visible signs of trauma and no scars or marks.
- her eyes are cloudy, which is something that usually only happens to bodies that have been dead for a few days, yet the corpse looks fresh.
- her wrist and ankle bones are shattered without any outward signs of injury.
- They extract from her nails and hair a kind of peat that is only naturally found in the northern U.S.
- her tongue has been non-surgically removed and one of her teeth is missing.
- her vagina was mutilated.
The internal examination
- the corpse bleeds profusely, something that usually only happens to fresh corpses.
- Tommy attributes her abnormally small waist to the use of a corset, which were commonly worn by women in the past.
- Austin discovers that the blood he stored in the freezer strangely started to leak.
- her lungs reveals that they are severely blackened, which is consistent with someone who has suffered third-degree burns
- Her internal organs reveal numerous cuts and scar tissue, likely from repeated stabbing.
- they find Jimsonweed (Datura stramonium) in Jane Doe's stomach, a paralyzing agent that, again, is only found in the north of the country.
- finds her missing tooth wrapped in a piece of cloth in her stomach. They find Roman numerals, letters, and a drawing on the cloth.
- When Tommy finally separates the skin on her chest from the body, they find similar symbols on the inside of her skin.
- Austin folds the piece of cloth and discovers the name of a passage from the Bible and that the Roman numerals read 1693. Tommy finds the corresponding passage in the Bible, Leviticus 20:27, that condemns witches. Austin concludes that she must be a witch who died during the Salem trials, since all of the evidence adds up. Tommy rebuts this by stating that those women were not actually witches, it was only a case of mass hysteria, and that her injuries are not similar to the methods used during the trials.


- 7:06:00 PM
- 0 Comments


Perks of being medical student?

I'm so hungry and my duit belanja for this month dah habis. I cannot go for groceries shopping. Hmm.


I just ate instant noodles for buka puasa just now. Well, it was delicious and I still hungry so I made a night snack to fulfil my monsterous appetite.

Taaaadaaaaaaaaaaaaaa, a bowl of milo oates :D




Someone should be baik hati and belanja me all these huwaaaaa ! (literally cry)
And he is still busy playing those games, I don't know why I need to compete with games for his attentions (facepalm)

So I currently studying in dining hall, using the dining table. I really love large, wide table because it has wider space for my laptop, my books, my stationary and yeaaa my phone, and also my lecture notes and so on. Messy type of people huh.

Yupppppp like theseeeeeeee, that's why I need wider, lager table. Get it now?

Seriously I love the background , stuck on the wall like that. But yeaa the desk is too small for me. Not for study, but yeaaa suit to watch movie from laptop or something.


I really love those kind of chair. I don't know why. Even in the Sim's Freeplay I bought that kind of chairs. Hahaha.

Buy me a Macbook please ! Sobs sobs..

- 11:39:00 PM
- 0 Comments

F E T A L
C I R C U L A T I O N


M U R M U R S
What is murmurs?
When normal laminar blood flow within the heart is disrupted, an audible sound is created by turbulent blood flow. Outside of the heart, audible turbulence is referred to as a bruit, whereas inside the heart it is called a murmur.
There are four major causes of cardiac murmurs:
- Valvular stenosis: If blood is forced through a tight area, turbulent blood flow ensues, as is the case in valvular stenosis. Generally, the worse the stenosis, the louder the murmur; however, if heart failure develops, adequate pressures to create turbulent blood flow may not be able to be achieved, and the murmur may lessen or even disappear. Thus, the intensity of a murmur is not used to indicated severity of disease.
- Valvular insufficiency: Blood abnormally travels backward through an incompetent valve in valvular insufficiency, causing turbulence when it meets normal, forward blood flow.
- Congenital anomaly: If blood is forced through a congenital anomaly from one chamber to another, as in an atrial septal defect (ASD) or ventricular septal defect (VSD), a murmur is produced — again due to turbulence.
- Increased blood flow: Yet another cause of cardiac murmurs is increased flow of blood through a normal valve. In high-output states such as anemia, thyrotoxicosis or sepsis, a large volume passes through the cardiac valves, and the normal laminar blood flow may be disturbed. Still's murmur is a normal aortic flow murmur frequently heard in childhood that frequently disappears over time.
Murmurs
by American Family Physician
Precordial Palpation
The cardiac examination begins with palpation to assess precordial activity and femoral pulses. Increased precordial activity is commonly felt in patients with increased right or left ventricular stroke volume. Increased pre-cordial activity occurs in patients with an atrial septal defect, a moderate or large ventricular septal defect or significant patent ductus arteriosus. This increased activity should raise the possibility that the auscultatory findings may be pathologic. Other explanations for increased precordial activity include patient anxiety, anemia and hyperthyroidism.
Once both brachial pulses have been palpated, the right brachial pulse should then be palpated simultaneously with the femoral pulse. If the timing and intensity of the two pulses are equal and blood pressure in the right arm is normal, coarctation of the aorta is unlikely.
Precordial palpation is also necessary to feel “thrills,” which are the palpable consequence of blood flowing rapidly from high pressure to lower pressure. Some ventricular septal defects result in thrills at the lower left sternal border. Moderate to severe pulmonary valve stenosis may cause a thrill at the upper left sternal border. A thrill resulting from aortic stenosis is frequently palpable in the suprasternal notch.
Auscultation of First and Second Heart Sounds
Precordial palpation is followed by auscultation. This part of the examination entails separate evaluation of each heart sound and each phase of the cardiac cycle.
FIRST HEART SOUND
Auscultation begins with listening for the first heart sound (S1) at the lower left border of the sternum. The S1 is caused by closure of the mitral and tricuspid valves and is normally a single sound. An inaudible S1 indicates that some sound is obscuring the closure sound of these valves. The differential diagnosis for murmurs that obscure S1 includes ventricular septal defects, some murmurs caused by atrioventricular valve regurgitation, patent ductus arteriosus and, occasionally, severe pulmonary valve stenosis in a young child. These S1-coincident murmurs are also known as “holosystolic” murmurs.
CLICKS
If S1 is audible but appears to have two components at some spots in the precordium, the patient has either a click or an asynchronous closure of the mitral and tricuspid valves. Clicks may originate from any valve in the heart. Depending on their origin, clicks have different identifying characteristics.
Ejection clicks originating from the pulmonic valve begin shortly after the atrioventricular valves close, vary with respiration and are best heard at the upper to middle area of the left sternal border. Aortic valve ejection clicks begin shortly after S1 and are best heard at the apex. They do not vary with respiration.
Systolic clicks originating from the mitral valve are best heard at the apical area when the patient is standing. Occasionally, the tissue closing a ventricular septal defect can pop or click early in systole.
SECOND HEART SOUND
After auscultation for clicks throughout the four listening areas, the next step is to return to the upper left sternal border and listen to the second heart sound (S2). This sound is caused by closure of the aortic and pulmonic valves.
The S2 should split into two components when the patient inspires. The first component, aortic second sound (A2), is closure of the aortic valve. The second component, pulmonic second sound (P2), is caused by closure of the pulmonary valve. The splitting of S2 occurs because inspiration brings more blood into the right ventricle. Right ventricular ejection is prolonged, and the pulmonary valve closes later. An awareness of this phenomenon is helpful in understanding the physical examination features of the patient with an atrial septal defect. A loud, single S2 indicates either pulmonary hypertension or congenital heart disease involving one of the semilunar valves.
Murmurs
Systolic murmurs have only a few possible causes: blood flow across an outflow tract (pulmonary or aortic), a ventricular septal defect; atrioventricular valve regurgitation, or persistent patency of the arterial duct (ductus arteriosus). Systolic murmurs can also be functional (benign).
GRADES
Systolic murmurs are graded on a six-point scale. A grade 1 murmur is barely audible, a grade 2 murmur is louder and a grade 3 murmur is loud but not accompanied by a thrill. A grade 4 murmur is loud and associated with a palpable thrill. A grade 5 murmur is associated with a thrill, and the murmur can be heard with the stethoscope partially off the chest. Finally, the grade 6 murmur is audible without a stethoscope. All murmurs louder than grade 3 are pathologic.
TIMING
Systolic murmurs may be timed as early, middle or late systolic. They can also be timed as holosystolic.
VENOUS HUMS
Many children with functional murmurs have venous hums. These sounds are caused by the flow of venous blood from the head and neck into the thorax. They are heard continuously when the child is sitting. The sounds should disappear when light pressure is applied over the jugular vein, when the child's head is turned or when the child is lying supine. Venous hums are common and are not pathologic. Patients with venous hums do not require pediatric cardiology referral. All other diastolic murmurs are pathologic and therefore warrant referral.
DESCRIPTION OF CHARACTER
The character, or tone, of a murmur may aid in the diagnosis. Words such as “harsh,” “whooping,” “honking,” “blowing,” “musical” and “vibratory” may be useful, albeit somewhat subjective, in describing murmurs.
A “harsh” murmur is consistent with high-velocity blood flow from a higher pressure to a lower pressure. “Harsh” is often appropriate for describing the murmur in patients with significant semilunar valve stenosis or a ventricular septal defect.
“Whooping” or “blowing” murmurs at the apex occur with mitral valve regurgitation. The term “flow murmur” is often used to describe a crescendo/decrescendo murmur that is heard in patients with a functional murmur. However, similar systolic ejection murmurs may be heard in patients with atrial septal defect, mild semilunar valve stenosis, subaortic obstruction, coarctation of the aorta or some very large ventricular septal defects.
Many functional or innocent murmurs are “vibratory” or “musical” in quality. Still's murmur is the innocent murmur most frequently encountered in children. This murmur is usually vibratory or musical.
LOCATION OF HIGHEST INTENSITY
The location of the highest intensity of a murmur is also important (Table 1). A murmur caused by aortic stenosis is often best heard at the upper sternal border, usually on the right side. A murmur resulting from pulmonary stenosis is heard best at the upper left sternal border. A murmur caused by a ventricular septal defect or tricuspid valve insufficiency is heard at the lower left sternal border. A murmur resulting from mitral valve regurgitation is best heard at the apex.
TABLE 1
Listening Areas for Common Pediatric Heart Murmurs
| AREA | MURMUR |
|---|---|
Upper right sternal border
|
Aortic stenosis, venous hum
|
Upper left sternal border
|
Pulmonary stenosis, pulmonary flow murmurs, atrial septal defect, patent ductus arteriosus
|
Lower left sternal border
|
Still's murmur, ventricular septal defect, tricuspid valve regurgitation, hypertrophic cardiomyopathy, subaortic stenosis
|
Apex
|
Mitral valve regurgitation
|
POSITION CHANGES IN THE DIFFERENTIATION OF MURMURS
Position changes are very helpful in differentiating functional and pathologic murmurs. The vibratory functional murmur heard in a young child (Still's murmur) decreases in intensity when the patient stands.
Most pathologic murmurs do not change significantly with standing. An important exception is the murmur of hypertrophic cardiomyopathy, a potentially life-threatening condition. This murmur increases in intensity when the patient stands. In the upright position, venous return to the heart is reduced, decreasing the left ventricular end diastolic volume. As left ventricular size decreases, the left ventricular outflow tract narrows, and the systolic outflow obstruction increases. This narrowing increases the intensity of the murmur. Overall, hypertrophic cardiomyopathy is rare; however, it is one of the leading causes of sudden death in athletes.
Atrial Septal Defect
Perhaps the best way to decide whether a patient needs to be referred to a pediatric cardiologist is to know confidently the clinical findings of the atrial septal defect. The abnormal findings in patients with atrial septal defects are often quite subtle and thus are easily confused with the physical findings in patients with functional or innocent murmurs (Table 2). Loud murmurs from ventricular septal defects or significant aortic or pulmonic stenosis are not subtle and are not often confused with innocent murmurs.
TABLE 2
Physical Findings in Functional (Innocent) Heart Murmur and Atrial Septal Defect
| PHYSICAL FINDING | INNOCENT MURMUR | ATRIAL SEPTAL DEFECT |
|---|---|---|
Precordial activity
|
Normal
|
Increased
|
First heart sound (S1)
|
Normal
|
Normal
|
Second heart sound (S2)
|
Splits and moves with respiration
|
Widely split and fixed (i.e., does not move with inspiration)
|
Systolic murmur (supine)
|
Crescendo/decrescendo
|
Crescendo/decrescendo
|
Possibly vibratory at lower left sternal border
|
“Flow” at upper left sternal border
| |
Systolic murmur (standing)
|
Decreases in intensity
|
Does not change
|
Diastolic murmur
|
Venous hum
|
Inflow “rumble” across tricuspid valve area
|
The first step in the examination is palpation for the precordial activity at the left sternal border, feeling for increased activity that may be present from right ventricular enlargement. The examination is performed with the patient in a supine position.
Auscultation at the lower left sternal border should reveal a normal, single and easily audible S1. Listening at the upper left sternal border for S2 should reveal variable splitting with respiration. A widely split S2 that does not change with respiration indicates either complete right bundle branch block or an atrial septal defect.
Because of the increased volume of blood in the right ventricle in the patient with an atrial septal defect, the S2 always sounds as if the patient has taken a deep breath. This means that the volume of blood in the right ventricle is increased and it takes longer for the ventricle to eject its contents, thus leading to a fixed, widely split S2.
Murmurs heard in patients with atrial septal defects are often of low pitch and intensity. However, the intensity of the murmur is not a reliable basis for the diagnosis. The systolic murmur is caused by an increased volume of blood coursing across the right ventricular outflow tract. If the murmur is audible, it can be heard at the upper left sternal border.
Patients with atrial septal defects may also have a diastolic murmur. In this situation, increased diastolic blood flow across the tricuspid valve may cause a soft, often barely audible low-frequency “diastolic rumble.” This sound is heard best with the bell of the stethoscope placed at the lower left sternal border. Pushing down with the bell causes the skin beneath the stethoscope to act as a diaphragm. Consequently, only the high-frequency sounds are heard. Releasing the tension on the bell allows the low-frequency rumbling sound to become audible at the lower left sternal border.
After the supine examination, the examination should be repeated with the patient standing. If the patient has an atrial septal defect, the features of increased precordial activity, a widely split S2, a systolic murmur at the upper left sternal border and a diastolic rumble should still be present when the patient is standing. If the patient has an innocent or functional murmur, the precordial activity should be normal, the S2 should split and move with respiration, the systolic murmur should decrease in intensity and no diastolic murmur should be present in the tricuspid valve area.
If no symptoms are present, the S1 is normal, the S2 splits and is of normal intensity, and no clicks are heard, the differential diagnosis of a grade 1 to grade 2 systolic murmur is frequently a choice between an atrial septal defect and a functional murmur.
In young children, it can be difficult to confidently distinguish the respiratory variation of S2 splitting in the patient with a normal murmur from the fixed S2 splitting in the patient with an atrial septal defect. Because the patient with an asymptomatic atrial septal defect will not develop pulmonary hypertension or other permanent sequelae early in life, careful yearly follow-up examination by the primary care physician can be recommended. By the time a child reaches preschool age, the normal or abnormal splitting of the S2 usually becomes clear (Table 3).
TABLE 3
Features That Increase the Likelihood of Cardiac Pathology
Symptoms such as chest pain
|
Family history of Marfan syndrome or sudden death in young family members
|
Malformation syndrome (e.g., Down syndrome)
|
Increased precordial activity
|
Decreased femoral pulses
|
Abnormal second heart sound
|
Clicks
|
Loud or harsh murmur
|
Increased intensity of murmur when patient stands
|
The Authors
MICHAEL E. MCCONNELL, M.D., is associate professor of pediatrics at East Carolina University School of Medicine, Greenville, N.C. Dr. McConnell received his medical degree from the University of Alabama School of Medicine, Birmingham. He completed a pediatric residency at Children's Hospital, Birmingham, Ala., and a fellowship in pediatric cardiology at Children's Hospital Medical Center, Cincinnati.
SAMUEL B. ADKINS III, M.D., is assistant residency director and director of primary care sports medicine for the family practice residency program at East Carolina University School of Medicine. Dr. Adkins graduated from the University of Pittsburgh School of Medicine and completed a residency in family practice at St. Margaret Memorial Hospital, Pittsburgh.
DAVID W. HANNON, M.D., is associate professor of pediatrics at East Carolina University School of Medicine. Dr. Hannon received his medical degree from the University of South Florida College of Medicine, Tampa, and completed a pediatric residency and a cardiology fellowship at Children's Hospital Medical Center, Cincinnati.
REFERENCES
hide references
1. Rosenthal A. How to distinguish between innocent and pathologic murmurs in childhood. Pediatr Clin North Am. 1984;31:1229–40.
2. McCrindle BW, Shaffer KM, Kan JS, Zahka KG, Rowe SA, Kidd L. Factors prompting referral for cardiology evaluation of heart murmurs in children [Letter]. Arch Pediatr Adolesc Med. 1995;149:1277–9.
3. Danford DA, Nasir A, Gumbiner C. Cost assessment of the evaluation of heart murmurs in children. Pediatrics. 1993;91:365–8.
4. Hurwitz RA, Caldwell RL. Should pediatric echocardiography be performed in adult laboratories? [Abstract] Pediatrics 1998;102:390. Complete text at e15 at: www.pediatrics.org.
5. Pelech AN. The cardiac murmur: when to refer? Pediatr Clin North Am. 1998;45:107–22.
6. Maron BJ, Epstein SE, Roberts WC. Causes of sudden death in competitive athletes. J Am Coll Cardiol. 1986;7:204–14.

Findings

- 8:54:00 PM
- 0 Comments














