
Chest Pain Differential Diagnosis
2:14:00 AM


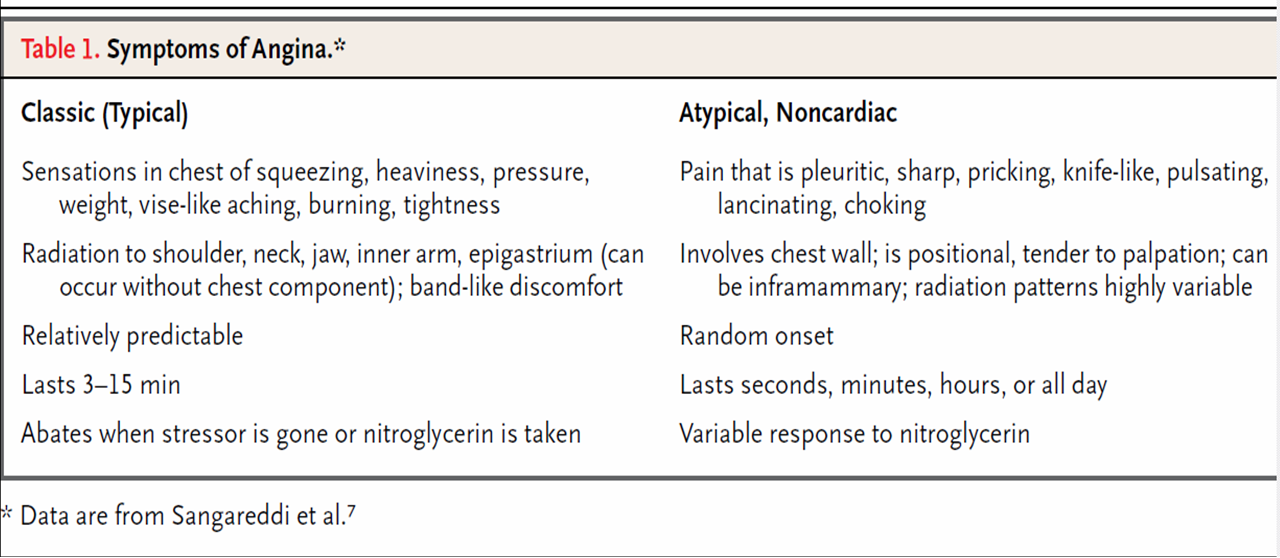
Distinguishing between Cardiac and Non-Cardiac Chest Pain
There is no conclusive way to differentiate between cardiac and non-cardiac chest pain in the home environment. There are many cases where severe heartburn causes chest pain that resembles cardiac disease and only the use of nitrates may allow a person to differentiate between cardiac and non-cardiac chest pain in this instance. Severe chest pain should always be taken seriously and a trip to the emergency room is often warranted to exclude more serious underlying disorders. This can only be done under the supervision of a medical professional in conjunction with the relevant tests and investigations. Refer to Chest Pain Tests and Chest Pain Diagnosis for more information.
Nature
- Cardiac
- Pain is dull, constricting, choking and/or crushing.
- Other terms to describe ischemic cardiac chest pain includes squeezing, burning or heavy.
- Sometimes it may just feel like discomfort which is why the character of cardiac chest pain can be so misleading.
- A common but inconclusive presentation in cardiac chest pain is a patient clutching the chest
- Non-Cardiac
- The pain may vary from burning to sharp, stabbing and prickling.
- Chest pain due to anxiety may also result in pain that is similar to cardiac chest pain.
Location
- Cardiac
- The pain is usually central (towards the center of the chest) and fanning outwards (diffuse).
- Non-Cardiac
- Pain may be away from the center of the chest where a patient can clearly identify it as a right-sided or left-sided chest pain.
- Pain is usually localized – located at only one spot which can be clearly pinpointed by the patient.
Radiation
- Cardiac
- Pain to the jaw, neck, shoulder, arms (either one or even both) or back.
- Sometimes there pain may be radiated to the upper abdomen.
- Non-Cardiac
- There may not often be any radiation of the pain or it may radiate to other sites apart from those mentioned above.
- Gastritis with accompanying GERD may cause a burning chest pain as well as upper abdominal pain and this may be confused for radiation.
Precipitating Factors
- Cardiac
- Triggered or exacerbated by exertion or emotion.
- At times a large meal or even extremes of temperature, particularly cold, can trigger or exacerbate the pain.
- Unstable angina may not be triggered by any specific factors.
- Non-Cardiac
- Spontaneous although it may be exacerbated by exertion (usually after rather than during activity).
- Changes in posture, deep or rapid breathing or pressure may also exacerbate the pain.
Relieving Factors
- Cardiac
- Pain is relieved by rest and responds quickly to nitrates.
- Non-Cardiac
- Not relieved significantly by rest, if at all.
- Does not respond to nitrates or there may be a slow response.
- Pain relived by antacids may be related to gastrointestinal disorders. Pain that improves upon leaning forward may be related to the pericarditis (inflammation of the lining around the heart).
Concomitant/Associated Signs and Symptoms
- Cardiac
- Severe shortness of breath – patient may report a feeling of suffocation.
- Dizziness
- Fainting spells (‘blackouts’)
- Non-Cardiac
- Other signs and symptom may be present that is helpful in identifying the cause of the pain.
- Gastrointestinal – bloating, belching, nausea, vomiting and/or regurgitation. Refer to Gastric Chest Pain.
- Respiratory – shallow breathing, persistent cough, abnormal breathing sounds, difficulty breathing when lying flat, expectorating mucus or coughing up blood. Refer to Lung Chest Pain.
- Musculoskeletal – limited range of motion, cannot tolerate pressure on the affected area. Refer to Muscle Chest Pain and Bone Chest Pain.
- Psychological – weepy, depressed, excited, agitated, fearful. Refer to Nerve Chest Pain.
























0 comments